Surgeon Q&A: Surgical & Transcatheter Aortic Valve Insights with Dr. Joanna Chikwe
Written By: Adam Pick, Patient Advocate, Author and Website Founder
Medical Expert: Joanna Chikwe, MD, Chair of Cardiac Surgery, Cedar-Sinai Medical Center
Published: June 27, 2024
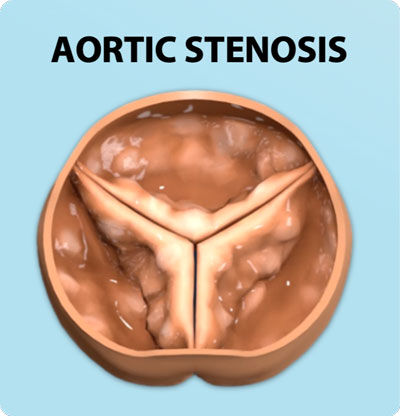
A new or unexpected diagnosis of a failing aortic valve can be stressful and frightening. More than anything, the fear often comes from not knowing the next steps for the optimal treatment of life-threatening diseases including aortic stenosis. However, Patients should know that, during the past 50 years, aortic valve surgery has greatly advanced. There are many treatment options that are safe and effective with minimal risk.
For example, there are minimally-invasive transcatheter aortic valve replacement (TAVR) procedures to treat aortic stenosis. While TAVR was initially designed for older, higher-risk patients, this revolutionary therapy is now acceptable for low-risk patients who often go home just one day after the procedure. There are also surgical aortic valve replacement (SAVR) approaches which require an incision to the patient’s chest or ribs. While the recovery from SAVR is longer, this may be a better option for younger patients for various reasons. As some of you know, I had a Ross Procedure nearly 20 years ago, which has worked out very well for me as I have not needed a re-operation.
One thing is for sure, there is no shortage of questions when it comes to aortic valve replacement. That’s why I was thrilled when Dr. Joanna Chikwe, Chair of Cardiac Surgery at Cedars-Sinai Medical Center, agreed to share her experience and insights about what patients need to know about TAVR and SAVR in the setting of heart valve surgery today.
Key Learnings About TAVR vs. SAVR in 2024
Here are important insights shared by Dr. Chikwe during our interview:
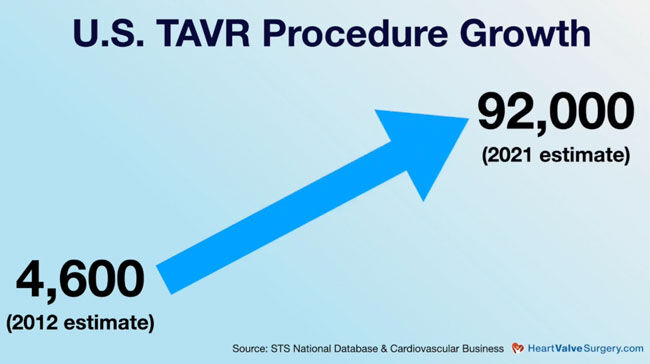
- The use of TAVR to treat aortic stenosis has grown significantly during the past 10 years. During 2023, there were over 100,000 TAVR procedures performed which is an exponential increase from the 4,000 TAVR procedures performed in 2012, according to The Society of Thoracic Surgeons.
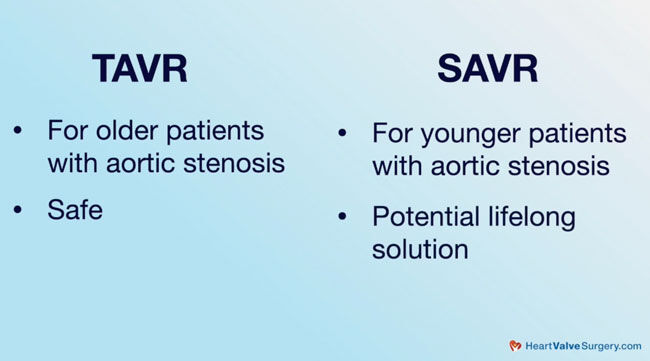
- TAVR is a safe and effective procedure typically used on older patients while SAVR is often used on younger patients. “TAVR, absolutely a great solution for older patients with tight aortic stenosis; super safe,” said Dr. Chikwe. “Surgery becomes a really important option for younger patients because they need lifelong solutions.”
- For younger patients, there are many options for the surgical treatment of aortic valve disease. Those therapies may include different types of SAVR including aortic valve repair, valve-sparing, and the Ross Procedure which enable patients to keep their own valve tissue. In addition, patients may opt for a mechanical heart valve replacement. “We want to think about better solutions,” Dr. Chikwe states. “For patients in their 20s, 30s, and 40s, we always talk about Ross procedure. That can give people the best freedom from the need for medications and other procedures. Some patients might be suitable for mechanical valve replacements. That’s not something we can do through a catheter.”
- Aortic valve patients with other cardiac conditions including aneurysms, atrial fibrillation and coronary artery disease need to be made aware of the opportunities and constraints for concomitant treatment. Dr. Chikwe states, “There are patients who have aneurysmal disease of the aorta and need a very specific and different approach because a TAVR isn’t the safest option for them.”
- When deciding on a valve replacement, planning what might happen in the future is necessary. Chikwe told us that planning for the future is a key part of the decision-making process. “We map out the implications of having a mechanical valve and needing anticoagulation, the long-term stroke risk, and the risk of re-operation,” she said. “If we choose to place a tissue valve, how can we set that patient up for success through potentially more than one procedure?”
- A tissue valve replacement provides patients more options if future aortic valve interventions are required including a surgical re-replacement. Dr. Chikwe shared that, in terms of having a tissue valve replacement, it’s much better to be able to plan for a redo aortic valve surgery down the road. Even though another surgery may mean a patient will have a four or five-day hospital stay, it is a low-risk solution and much better than suffering the devastating complications of anticoagulation and stroke that can sometimes go along with a mechanical valve.
Thanks Dr. Chikwe and Cedars-Sinai Medical Center!
Thank you, Dr. Chikwe, for everything you and your team at Cedars-Sinai Medical Center in Los Angeles are doing for heart valve patients across the world!
Related links:
- See 50+ Patient Reviews for Dr. Chikwe
- Surgeon Q&A: How Is The Heart Stopped During Cardiac Surgery?
- Life Expectancy & Heart Valve Surgery: What Should You Know?
Keep on tickin!
Adam
P.S. For the deaf and hard-of-hearing members of our community, I have provided a written transcript of this video below.
Written by Adam Pick
- Patient & Website Founder

Video Transcript:
Adam Pick: Hi everybody, it’s Adam with heartvalvesurgery.com. Today we’re in Los Angeles. I’m thrilled to be joined by Dr. Joanna Chikwe, who is the founding chair of Cardiac Surgery at Cedars-Sinai Medical Center. Dr. Chikwe, it is great to see you again.
Dr. Chikwe: Great to see you, Adam.
Adam Pick: Yeah, we’re here in your office having some great conversations about valvular disease management treatment. One of the conversations was about TAVR (transcatheter aortic valve replacement) and SAVR (surgical aortic valve replacement). We were both amazed at this ramp in TAVR. I think last year, over 90,000 TAVRs were done, but at the same time, patients are still having a lot of their valves treated surgically. The big question for you is today, what should patients know about TAVR or SAVR?
Dr. Chikwe: TAVR, absolutely great solution for older patients with tight aortic stenosis; super safe. Surgery becomes a really important option for younger patients, and that’s because younger patients need lifelong solutions. We don’t just want to use biological valves which may wear out and need several more procedures, we want to think about better solutions. For patients in their 20s, 30s, 40s, we always talk about Ross procedure. That can give people, as you know, really the best freedom from needs for medications and other procedures. Some patients might be suitable for mechanical valve replacements, and that’s not something that can be done through a catheter. Then there are patients who have got aneurysmal disease of aorta and they need a very specific and different approach because a TAVR isn’t really the safest option for them.
Adam Pick: I appreciate. For those of you out there who don’t know, I had a Ross procedure done almost 18 years ago without re-operation. It has worked for me, but it’s not for everybody. I’m real curious to know, Dr. Chickwe, when you meet with patients, you reference the lifelong management of valve disease. Is this something with every patient who comes through that door, you sit down and map out with them what might happen down the road?
Dr. Chikwe: We absolutely do because it’s such a key part of the decision making. We also map out what are the implications of having a mechanical valve and needing anti-coagulation, what is the stroke risk long term, as well as what is the risk of re-operation. If we choose to place a tissue valve, how can we set that patient up for success through potentially more than one procedure? Always remembering that to redo aortic valve surgery, four or five days in the hospital, super low risk, something you can plan. It’s nothing like as devastating as the complications of mechanical valves anti-coagulation stroke.
Adam Pick: Dr. Chikwe, on behalf of all the patients at heartvalvesurgery.com, patients all over the world, thanks for everything you are doing here at Cedars-Sinai in Los Angeles.
Dr. Chikwe: Thank you, Adam.
Adam Pick: Hi everybody, it’s Adam. I hope you enjoyed that video. Don’t forget, you can always subscribe to our YouTube channel. Watch the next two educational videos coming up on your screen or click the blue button to visit heartvalvesurgery.com.